
England’s Stroke Centres Fail to Meet 24/7 Mechanical Thrombectomy Pledge
It is a sobering thought for anyone living in a bustling metropolis like Chicago, where we often assume that the proximity of world-class medical facilities guarantees immediate, life-saving care. But a recent exclusive report out of England serves as a stark reminder that the gap between a government’s promise and the reality of the hospital ward can be a matter of life and death. In the UK, the National Health Service (NHS) has failed to meet a critical deadline to provide 24/7 access to a “game-changing” stroke treatment, leaving patients in underserved areas vulnerable during the overnight hours and weekends.
The Critical Failure of 24/7 Stroke Care
The treatment in question is mechanical thrombectomy, a sophisticated clot-removal technique designed to mitigate the devastating effects of a severe stroke. According to recent reports, the NHS was expected to ensure this procedure was available around the clock across all regional stroke centres in England starting April 1. Still, the reality on the ground is far different. Seven of the 24 regional stroke centres are still unable to provide this service 24/7.
The reason cited is a systemic one: a lack of doctors and specialized staff. While ministers had repeatedly pledged that this life-changing intervention would be universal, the staffing shortages have created a dangerous lottery based on geography and timing. For a resident of a city like Chicago, this highlights a universal anxiety—the fear that if a medical emergency strikes at 3:00 AM on a Sunday, the necessary specialist might not be on call, regardless of how “advanced” the hospital claims to be. You can read more about how these systemic gaps affect emergency care standards in urban environments.
Understanding the Stakes: Why Timing is Everything
To understand why the failure to provide 24/7 access is so catastrophic, one has to look at the nature of an ischaemic stroke. This occurs when a blood vessel is blocked by a clot, effectively cutting off the oxygen supply to a portion of the brain. Without that oxygen, brain cells begin to die rapidly. In the UK alone, more than 100,000 people suffer a stroke annually, with 38,000 resulting in death and countless others facing life-changing disabilities that strip away their independence.
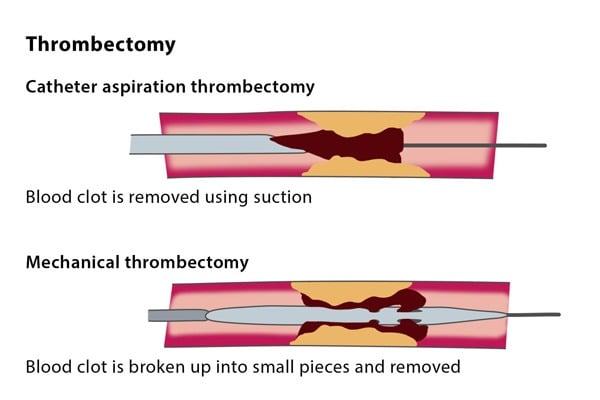
Mechanical thrombectomy is described by medical professionals as a game-changer because it allows for the physical removal of the clot. This is a specialized emergency procedure led by an Interventional Neuroradiologist, who uses guidewires and specialized equipment to clear the artery and restore blood flow. When performed quickly, it can prevent a patient from ending up with a serious, permanent disability.
Thrombectomy vs. Thrombolysis: The Race Against the Clock
It is important to distinguish between the two primary ways doctors handle these clots. First, there is thrombolysis, which involves the administration of a “clot-busting” medication known as a thrombolytic agent. This is delivered via a needle in the vein (venflon) to dissolve the blockage. However, thrombolysis is incredibly time-sensitive; it is most potent when administered within 3 to 4.5 hours after the onset of symptoms. Not every patient is a candidate for this medication due to associated risks.
This is where mechanical thrombectomy becomes the essential fallback and primary tool for severe blockages. If a clot is blocking a major vessel, thrombolysis is often done in conjunction with thrombectomy. But if the medication isn’t feasible or fails, thrombectomy is the only known better alternative to remove the clot. If a patient arrives at a centre that cannot perform this procedure overnight, their symptoms may worsen, leading to avoidable disability or death.
Navigating Local Care in Chicago
While the current crisis is unfolding within the NHS in England, the lesson for those of us in the Chicago area—from the high-rises of the Loop to the neighborhoods along Lake Shore Drive—is to be proactive about where we go during a neurological emergency. Given my background in analyzing healthcare infrastructure, I believe it is vital for residents to know exactly what criteria to look for in local providers to ensure they aren’t victims of a “staffing gap” during off-hours.
If you are evaluating the stroke preparedness of your local healthcare network or seeking stroke recovery resources, here are the three types of local professionals and institutions you should prioritize:
- Board-Certified Interventional Neuroradiologists
- These are the specialists who actually perform the mechanical thrombectomy. When vetting a provider, do not just inquire if the hospital “offers” the service. Ask specifically if they have a dedicated Interventional Neuroradiology team on-site 24/7, or if they rely on an “on-call” system that may involve significant delays in getting the specialist into the operating room.
- Comprehensive Stroke Centers (CSC)
- Not all hospitals are created equal. You want to identify facilities designated as Comprehensive Stroke Centers rather than Primary Stroke Centers. A CSC is required to have the infrastructure for both thrombolysis and mechanical thrombectomy, along with specialized neuro-ICU care. Ensure the facility has a proven track record of handling acute ischaemic strokes during weekends and overnight shifts.
- Neuro-Rehabilitation Specialists
- Because strokes often lead to life-changing disabilities, the care doesn’t end with the removal of the clot. Look for rehabilitation specialists who specialize in neuro-plasticity and stroke recovery. The key criteria here are multidisciplinary teams—including physical, occupational, and speech therapists—who coordinate care specifically for brain injury patients rather than general orthopedic recovery.
Ready to locate trusted professionals? Browse our complete directory of top-rated stroke,nhs,hospitals,health,england,uknews,society experts in the Chicago area today.