
Mammary Duct Ectasia as MRI Non-Mass Enhancement in RAD51C Carrier With Pituitary Adenoma
Medical breakthroughs often feel like they happen in a vacuum, tucked away in academic journals, but for residents across the Chicago metropolitan area, the intersection of genetics and endocrine health is a very real, local concern. When we witness reports like the recent case in Cureus regarding mammary duct ectasia presenting as MRI non-mass enhancement—particularly in a patient who is a RAD51C carrier and has a pituitary adenoma—it highlights a complex diagnostic puzzle. For those navigating the healthcare landscape from the Magnificent Mile to the suburbs of Naperville, understanding how these disparate conditions—a genetic mutation, a pituitary tumor, and breast inflammation—interact is crucial for proactive health management.
The Complex Interplay of Pituitary Function and Breast Health
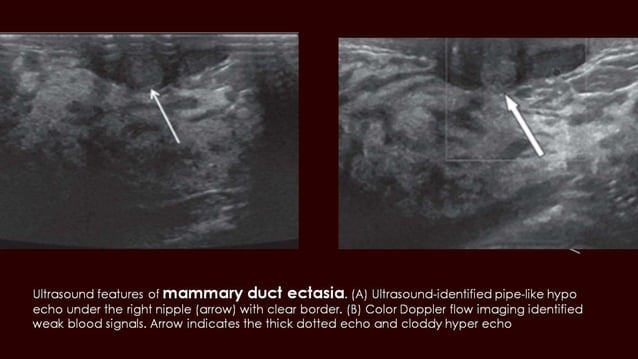
At first glance, a pituitary adenoma and mammary duct ectasia (MDE) might seem unrelated. Though, the clinical evidence suggests a deeper connection. Mammary duct ectasia is an inflammatory condition characterized by the dilation of major ducts and periductal inflammation. According to medical literature, there appears to be a relationship between certain hypothalamic or pituitary disorders and the development of MDE, specifically those related to prolactin secretion. In some cases, postmenopausal patients with pituitary chromophobe adenomas have developed bilateral duct ectasia, sometimes years after a hypophysectomy.
The role of prolactin is central here. Prolactin-producing pituitary adenomas can lead to hormonal imbalances that manifest in the breast tissue. In documented cases, MDE has developed both before and during the use of bromocriptine, a medication typically prescribed to manage prolactin levels. The pathology often involves marked ectasia affecting all excised ducts, sometimes accompanied by extensive cholesterol granulomas. For a patient in Chicago, this means that a “non-mass enhancement” seen on an MRI—which often triggers alarms for malignancy—might actually be a manifestation of this inflammatory process, complicated further by the patient’s genetic profile.
The RAD51C Variable and Diagnostic Challenges
The presence of a RAD51C mutation adds a significant layer of complexity. RAD51C is a gene associated with an increased susceptibility to certain cancers. When a patient carries this mutation, clinicians are naturally more vigilant, and the discovery of “non-mass enhancement” on a breast MRI is often viewed through the lens of high-risk screening. This creates a diagnostic tension: is the MRI finding a sign of a malignancy related to the RAD51C mutation, or is it a benign, albeit complex, manifestation of mammary duct ectasia driven by a pituitary adenoma?
This is where the multidisciplinary approach becomes vital. In a city with world-class medical hubs, the coordination between endocrinologists, genetic counselors, and radiologists is the only way to avoid unnecessary invasive procedures. The goal is to differentiate between the inflammatory changes of MDE and the proliferative changes that might signal a tumor. Understanding that pituitary dysfunction can mimic or mask other breast pathologies is a critical piece of the puzzle for anyone managing high-risk genetic markers.
Navigating Local Specialized Care in Chicago
Given the intricate nature of these overlapping conditions, relying on a general practitioner is rarely enough. If you are dealing with a combination of endocrine disorders and genetic predispositions, you need a specialized team. In my experience analyzing health trends, the key is finding providers who operate at the intersection of these fields rather than in silos. If you are managing these risks within the Chicago area, here are the three types of local professionals Make sure to prioritize.
- High-Risk Breast Imaging Specialists
- You need radiologists who specialize in “non-mass enhancement” interpretation. Look for providers affiliated with major academic medical centers who have specific experience with RAD51C or BRCA carriers. They should be capable of distinguishing between inflammatory ectasia and neoplastic growth, utilizing the latest MRI protocols to reduce false positives.
- Neuro-Endocrinologists
- Since the pituitary gland is the driver in these cases, a standard endocrinologist may not be sufficient. Seek a neuro-endocrinologist who specializes in pituitary adenomas and prolactin-secreting tumors. The criteria for a top provider here is their experience in managing the long-term hormonal fallout of hypophysectomies and their ability to coordinate with breast health teams.
- Certified Genetic Counselors
- For those with RAD51C mutations, a genetic counselor is essential for translating raw data into a clinical management plan. Ensure the counselor is experienced in “cascade testing” and can provide a personalized surveillance schedule that accounts for both the genetic risk and any existing endocrine comorbidities.
Managing a diagnosis that spans from the brain to the breast requires a level of coordination that can be overwhelming. By focusing on these specific archetypes of care, residents can ensure that their diagnostic journey is guided by expertise rather than anxiety. For more information on managing hereditary risks, you can explore our comprehensive health and wellness guides to better understand preventative screenings.
Ready to find trusted professionals? Browse our complete directory of top-rated medical experts in the chicago area today.